
April 21, 2026
In a Nutshell
- The federal government is actively pulling back from its role as a coordinating force for health expertise, guidance, and data collection.
- States have begun forming health alliances to perform some of the functions formerly performed by the federal government as well as those the federal government has started to do in ways that contradict established science.
- Michigan has not joined any of the existing alliances, despite strong incentives to prioritize health outcomes for its residents, and should consider joining one or leading its own.
The last year has been marked by significant changes in federal health policy. Previous work by the Research Council has highlighted changing policy regarding vaccination guidance, scientific and medical research funding, Medicaid, and the Affordable Care Act marketplaces. These changes exist within a broader context of the federal government spending less on public health insurance programs, but also pulling back from its role as a coordinating force for health expertise, guidance, and data collection.
Much attention has focused on changes to vaccine recommendations and controversial messaging from the federal government about Tylenol use during pregnancy causing autism. But, a big part of the story is the Trump Administration curtailing the overall capacity and role of the federal government to address major health policy issues. To date, the administration has cut over 20,000 jobs from the federal Health and Human Services Department workforce , including roughly 3,000 positions in the Centers for Disease Control and Prevention (CDC).
In the absence of federal leadership in some cases, states have been considering what they can do to fill the gaps. One idea that has emerged is the formation of state alliances or collaboratives to perform as many of the necessary functions as possible. Michigan has not joined any of the major state alliances, but should consider doing so or take the lead to establish one for the Great Lakes states.
State Health Alliances and Collaboratives
Over the last few months, three state partnerships have been announced to respond to the changing nature of federal health policy. These include the West Coast Health Alliance (WCHA), the Northeast Public Health Collaborative (NPHC), and the Governors Public Health Alliance (GPHA).
States That Have Joined At Least One Health Alliance in 2025
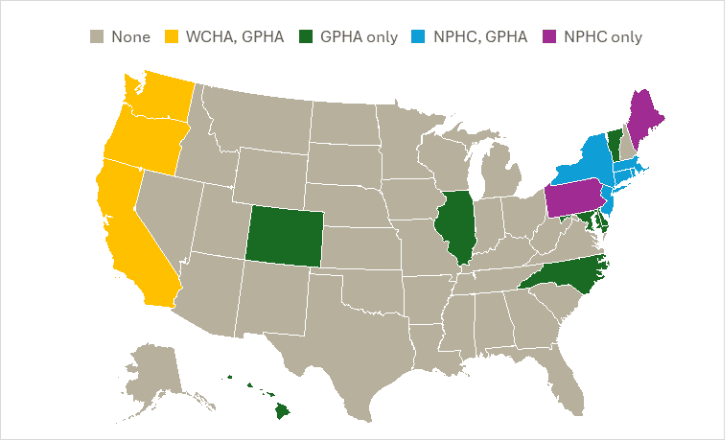
Source: Data compiled by Citizens Research Council from Alliance/Collaborative press releases. Note: Guam is also a member of the Governors Public Health Alliance
The purposes of these alliances are thematically similar.
- The West Coast Health Alliance seeks to ensure “that public health recommendations are guided by safety, efficacy, transparency, access, and trust” and wants to “safeguard scientific expertise by ensuring that public health policies in California, Oregon, and Washington are informed by trusted scientists, clinicians, and other public health leaders.”
- The Northeast Public Health Collaborative outlines a slightly broader mission, seeking “to share expertise, improve coordination, enhance capacity, strengthen regional readiness, and promote and protect evidence-based public health” as well as “optimizing the use of shared resources, innovating and reimagining core services – to ensure trust in public health, respond to public health threats, advance community health and strengthen confidence in vaccines and science-based medicine.”
- The Governors Public Health Alliance aims to “serve as a nonpartisan coordinating hub for governors and their public health leaders” and facilitate “data sharing and communication about health threat detection, emergency preparedness and response, public health guidance and policy, and deployment of experts.”
The Need for State-Level Public Health Alliances
The newly formed state alliances aim to fill an important and practical void left by the federal government. Non-member state governments also should be taking those abandoned functions seriously.
As the Research Council has highlighted in the context of vaccines and research funding, key features of public health policy often derive from federal action. Under the United States’ current model of federalism, it is often more efficient to centralize certain functions and services rather than having 50 states replicate the work. States may choose to effectuate vaccine requirements differently based on their local contexts, but it is redundant to have 50 different state health departments studying the efficacy of a particular drug. Similarly, siloing off research funding within state borders would lead to significant duplicative administrative work that has no real value to pursuit of knowledge. In both of those cases, the Research Council identified collaboration with other states as a potential policy option as the federal government retreats from its traditional roles here.
This principle applies to many other health-related functions. Preemptively creating a multi-state alliance that can handle many of these issues as they arise is more efficient than trying to address them collectively as they come up. It is also certainly more efficient than every state trying to form its own version of the CDC. Some of the areas where this kind of partnership would be valuable include:
Health Messaging and Guidance: The federal government has historically been the leading voice on all sorts of health information. Given recent moves on vaccinations and Tylenol use during pregnancy, for example, it is reasonable for states to assume that federal recommendations on health issues may divert from the scientific consensus going forward. Having a strong, unified voice on these topics would benefit the public so that individuals do not have to hunt for guidance from a trusted source.
Resource Pooling: Both in terms of money and information, being able to put the resources of many states together has significant value. This could play out in funding research, purchasing equipment or drugs, and studying important health problems. States will inevitably need to make their own decisions about how they use certain resources or deploy certain information within their borders, but states should have ways to share their resources efficiently when their collective efforts can produce better results than the sum of their individual ones.
Disease Monitoring: In the event of a major contagious disease outbreak, knowing what is happening around the country is vital to addressing the crisis. Given the federal government’s posture toward data integrity, particularly in the way current leaders speak about COVID and vaccine efficacy, states would be right to worry that CDC may not produce accurate information on a future pandemic. And even if states trust the federal government to prioritize accuracy, the staffing cuts at the CDC may limit states’ ability to do produce accurate information.
Disaster Response: States would benefit from having a mutual assistance framework in place that does not rely on federal coordination. States are used to helping each other when these issues arise, but it may be necessary to operate outside of the preexisting federal infrastructure.
Talent Capture: It is also worth highlighting the amount of expertise and talent that has been expelled from the federal government. Many of these talented and dedicated people may want to continue doing their work and have already shown a willingness to work in public service jobs, many for less salary than their market rate. States should be thinking about how to enlist these people into their workforces. Having a unified hub to bring these people into the state-level workforce would be a plus. Even if the ultimate outcome is these people landing state government health jobs, knowing they would be detailed to work on this collaborative project would likely be a selling point for those who have devoted their lives to this mission.
Entities are trying to fill the federal void and collaboration on these subjects is already happening. For instance, the Vaccine Integrity Project was formed to counterbalance the changes in federal vaccine policy. The American Academy of Pediatrics has broken with the CDC and issued its own recommendations as well. But without the centralized coordination functions that only states can provide, it is possible that duplication drains resources and the message gets lost in a sea of too many organizations trying to take the lead.
Michigan Needs the Alliances More than the Alliances Need Michigan
While it is likely that all states and the public they serve would benefit from participating in a state health alliance, Michigan is a state that cannot afford to fall further behind. The Research Council has documented how Michigan’s health outcomes lag behind the national and regional average across a host of metrics such as life expectancy, infant mortality, self-reported health status, and cardiovascular health. Conversely, one area where Michigan is doing better compared to other states is the share of the population that has some form of health insurance. That strength is imperiled by the recent Medicaid and Affordable Care Act changes, which are likely to decrease the share of the population that is covered and increase costs for those who retain coverage.
Michigan is also facing a tightening state budget environment. It would benefit greatly from joining a multi-state partnership that provides value to state residents without taxpayers having to cover the full cost of that work. Some may argue that many of the benefits of the alliances will be shared by non-member states (e.g., vaccine recommendations), but that will not be true for everything.
The state would likely incur some costs from joining one or more of these alliances, but the benefits seem clear. If the CDC did not exist five years ago, everyone would see the value in creating it. The federal government is a better venue for this work, but for now the states are the backstop.
Health Alliances Should Be Apolitical
So far, the alliances have only been joined by Democratic governors. Some may perceive partisan undertones in the announcements and coverage of the state health alliances, which is perhaps why governors in more evenly divided states, including Michigan, have not joined. However, the alliances seek to fill an important and practical void left by the federal government, regardless of the politics, and that makes it more important that states of all political leanings consider joining.
The functions in question here benefit the public at large and have generally been seen as nonpartisan in the past. The actions of these alliances will be shaped by their members, and their members should be as representative of the country as possible. The goal should be to establish a unified, consensus alliance.
A single health alliance that can perform the essential functions the federal government is abdicating would be ideal, but if Michigan is hesitant to join an existing alliance because it has concerns that the existing alliances are not apolitical, it could pick up the mantle and lead an alliance of Great Lakes states (these states include a mix of conservative, progressive, and “purple” states such as Michigan and Wisconsin).
Conclusion
The federal government is moving to spend less on public health insurance programs, but it is also pulling back from its role as a coordinating force for health expertise, guidance, and data collection. States have been considering what they should be doing to fill the gaps in health leadership, including formation of state alliances designed to perform as many of the necessary functions as possible.
For all of the reasons the CDC was originally formed, the states have a strong interest in maintaining an entity that pools monetary and intellectual resources toward maintaining public health and responding to crises.
Michigan has not joined any of the existing alliances, despite strong incentives to prioritize health outcomes in the state. If the state is not comfortable joining one of the existing alliances, it should consider spearheading the development of a regional alliance of its own.
