

December 4, 2025
In a Nutshell:
- Last week, the Citizens Research Council testified before the Michigan Senate Appropriations Subcommittee on Corrections and Judiciary about prisoner health care, an essential and expensive government function.
- The state has limited information about health outcomes, health care utilization, and health care costs within the state prison system, making it difficult to measure the adequacy and efficiency of care.
- Our 2023 report and the testimony suggested that the legislature should strongly consider mandating expanded data collection and reporting, ideally through a permanent statute.
Legislative oversight is an essential component of the law- and budget-making process. Without insight into the implementation and outcomes of existing policy, lawmakers are limited in their abilities to make effective decisions. Those insights are often informed by data. Data is a key piece of this information puzzle. Lawmakers need to be able to evaluate existing programs and understand the likely implications of making changes, and they cannot do so without good data. While this is true across the policy landscape, it is especially important for complex and expensive policy areas, as the consequences of poor program design and resource allocation are larger.
A central example in Michigan is the state’s prisoner health care system. The state has an obligation to prisoners and the public to provide constitutionally adequate care, but also to be a good steward of the $300 million annual expenditure of public money. The state must know whether it is providing appropriate care and how efficiently it is doing so. Answering those questions requires data, but it is data that the legislature – and even the Michigan Department of Corrections (MDOC) – does not currently have access to. That is the chief finding from our recent report examining health care in Michigan’s prisons, which the Citizens Research Council presented to the Michigan Senate Appropriations Subcommittee on Corrections and Judiciary last week (Video of testimony begins at 25:00). Improving legislative oversight in this area – and in many others – requires the legislature to mandate more expansive data collection.
Costs of Prison Health Care
An incarcerated person is essentially a ward of the state. Whether they are housed in public or private correctional facilities, the government is responsible for the care and well-being of prisoners, including providing health care. This obligation to provide health care flows from legal standards set by the U.S. and state constitutions, as well as federal and state laws, regulations, and policy. In addition to the obligation to prisoners to provide health care, governments – to protect themselves against litigation and waste – have concurrent obligations to the public to carry out their legal and ethical obligations in an effective manner while being good stewards of public resources. Beyond the general need for the prison health care system to provide constitutionally adequate care, prisoner health care also serves an important public safety function. Most prisoners will return to their communities, and it is in the public interest for formerly incarcerated people to be healthy and productive members of society who do not re-offend.
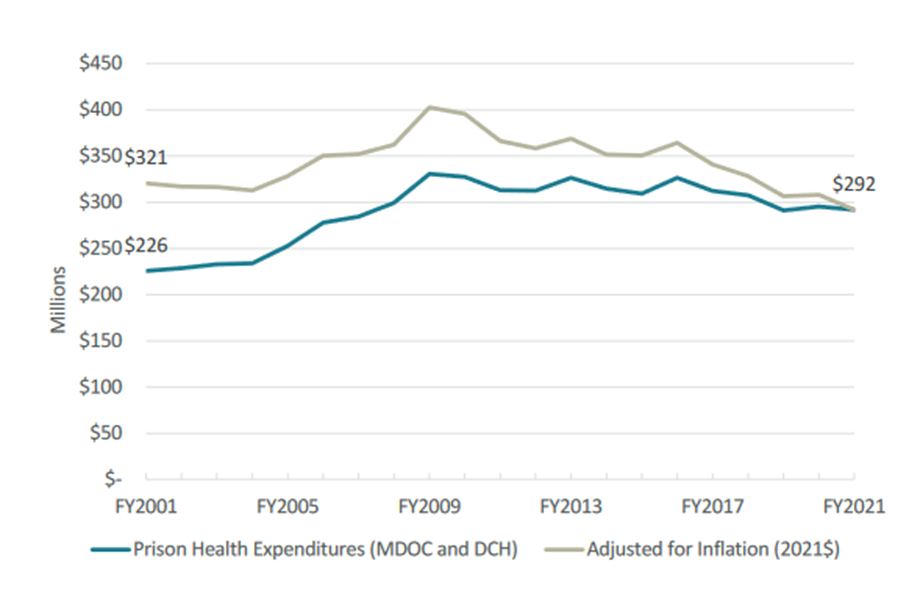
Prisoner health care is an essential function of state government, and it is an expensive one. In recent years, the state has spent around $300 million annually – between two and three percent of all general fund dollars – on prisoner health care. While the total costs have come down over the last decade, those declines are largely due to a decreasing prison population. On a per-prisoner basis, costs have climbed over the last two decades, even after adjusting for inflation.
Total Prison Health Care Expenditures in Michigan, FY2001 to FY2021
Source: Data compiled from MDOC Statistical Reports and U.S. Bureau of Labor Statistics Detroit CPI. Includes mental health expenditures by the Department of Community Health in state prisons prior to FY2011 when that line-item was transferred to the MDOC budget.
Per-Prisoner Health Care Expenditures in Michigan, FY2001 to FY2021
Source: Data compiled from MDOC Statistical Reports and U.S. Bureau of Labor Statistics Detroit CPI. Includes mental health expenditures by the Department of Community Health in state prisons prior to FY2011 when that line item was transferred to the MDOC budget.
The state has both a duty to and an interest in providing adequate health care in prison, but it also needs to keep a close eye on the cost of doing so, especially given the size of the prisoner health care line item.
Key Oversight Questions
Measuring success is an important part of any government initiative, but it is especially necessary for expensive public programs and services. The state needs to know if it is meeting its obligations to prisoners and the public, and how efficiently it is doing so. Specifically, the state needs to answer three general questions about prisoner health care:
- Is the state providing adequate care?
- Is the state providing care efficiently?
- What policy changes might be necessary to improve care and/or efficiency?
These are important questions for both the department and the legislature, but the legislature’s duty to conduct oversight over the laws it makes and the money it appropriates places it squarely in the center of this conversation.
Adequacy of Health Care in Prisons. For a variety of related reasons, the legislature needs information about the quality of the health provided in Michigan’s prisons. The legislature needs this information because failing to provide constitutionally adequate care comes with a host of financial and ethical costs, but also because it would undermine the state’s public safety goals. Relatedly, the legislature cannot properly analyze the efficiency of its prisoner health care spending without measuring the quality of the care itself.
Efficiency of Health Care in Prisons. The legislature needs information about how efficiently health care is being delivered in Michigan prisons. All government spending should be scrutinized to ensure that public money is being spent as efficiently as possible, but this is particularly important for large, complicated programs. Every year, the legislature is asked to appropriate a significant sum of money for prisoner health care and it needs to know how that money is being spent so it can evaluate whether modifications are necessary, either to the appropriation or the underlying laws.
Given that per-prisoner health care spending is on the rise, it is especially important for the legislature to study the efficiency of the system and its cost drivers.
Potential Policy Changes in Prison Health Care. Information on adequacy and efficiency of care is necessary for measuring the performance of the health care system and its contractors, but it is especially important for informing policymaking. If the prison health care system is not meeting the state’s goals and/or is not doing so efficiently, the legislature’s role is to step in with policy changes that would address the identified shortcomings. Without information on where the state stands and places for improvement, the legislature is unable to craft policy solutions to deal with any problems at hand.
Lack of Data on Prisoner Health Care
Despite the cost and importance of prisoner health care, the state possesses surprisingly limited data on prisoner health outcomes and the utilization and cost of health care for prisoners. While the department is required by appropriations boilerplate to publish some data, the required reports do not provide the information necessary to properly measure health outcomes, utilization, or cost to the degree necessary to conduct oversight and answer the key questions.
Data Needed on Health Outcomes. The legislature has access to very limited data on health outcomes for prisoners. While MDOC reports solid demographic data (e.g., age, sex, and race/ethnicity), the information it provides on the actual health status of prisons is lacking. The department provides some high-level talking points in presentations to the legislature each year, such as the total percentage of prisoners with mental health issues; total percentage of prisoners with substance abuse issues; number of pregnant prisoners; and number of prisoners being treated for cancer, but generally does not report anything comprehensive enough to measure health outcomes.
To properly assess health outcomes of prisoners, the department needs to track and report the following metrics, both upon entry into prison and over time:
- Percentage of prisoners with mental health issues broken down by severity and type/diagnosis
- Percentage of prisoners with substance abuse issues
- Percentage of prisoners with a chronic health condition (not just Hepatitis C) broken down by severity and type/diagnosis
- Percentage of prisoners considered overweight/obese
Data Needed on Health Care Utilization and Costs. In addition to the lack of data on health outcomes, the data on health care utilization and costs in Michigan’s prisons is also relatively sparse. State and national stakeholders have all theorized about rising per-prisoner health care costs, but there is limited data available to appropriately analyze what is driving the increasing costs. To properly understand whether the department is efficiently using its health care resources, the legislature needs significantly more data.
The most important data that the legislature needs on each cost-driver includes:
| Proposed Cost-Driver | Needed Data |
| General health care costs | Analysis of cost of supplies, tests, services |
| Mental Health | Breakdown of mental health conditions upon entry and over time Spending on mental health services by acuity/condition |
| Substance Abuse | Breakdown of substance abuse conditions upon entry and over time Spending on substance abuse services by type |
| Infectious Disease | Breakdown of the prevalence of different infectious diseases Spending on treatment of infectious disease by type |
| Preventative Care | Spending on preventative care Wellness exams and primary care visits per year |
| General Demand for Health Care | Overall metrics on the visits and services received across all categories (not just spending) |
| Specialty Care/In-Patient Care | Reasons for visits Total and per-visit costs Percent of prisoners utilizing these services |
| Prescription Drugs | Number of prisoners prescribed medication Total and per-unit costs |
| Aging Prisoners | Health care costs associated with each age group Service breakdown by age group |
| Staffing Shortages | Impact of shortages, such as delays in care |
This lack of data on health outcomes, utilization, and cost makes it essentially impossible for the legislature, and even the department, to make decisions about prisoner health care policy.
The Path Forward
The lack of information on prisoner health outcomes, health care utilization, and health care costs in prison makes it extremely challenging to answer the key oversight questions and make effective policies going forward. To make better policy, the legislature needs to ensure that the necessary data is being collected.
While data reporting requirements are frequently established during the annual appropriations process, the legislature should strongly consider codifying this data collection and reporting in statute. It is vital that the data is collected consistently from year to year and that the department has a clear, long-term mandate to build out its data collection and reporting infrastructure. Even if expanded data collection consistent with these recommendations made it into boilerplate next year, there is no guarantee it would survive year to year in identical form.
The fact that MDOC has changed software vendors and contractors on a regular basis also supports a broader, statutory requirement for data collection. Even if the data management software changes and the department loses access to older data, data from mandated statutory reports would be preserved and allow for comparisons across time.
This level of increased data collection and analysis would certainly come with administrative costs, but the potential for savings is likely to far exceed the staff and software costs associated with more data collection and reporting.
Conclusion
Prisoner health care is an essential and expensive government function. Despite the importance of adequate and efficient care, the state has very little information about health outcomes, health care utilization, and health care costs within the state prison system. This lack of information makes it difficult for both the department and the legislature to make and implement effective policy.
The first step in improving policy making in the prison health care system is for the legislature to mandate expanded data collection and reporting, ideally through a permanent statute. While there will be some administrative costs associated with doing so, the state cannot continue to have this little insight into the return on investment it receives on its $300 million prisoner health care system.
