
March 24, 2026
In a nutshell:
- Even as COVID-19 cases wane, Michigan hospitals lack the nurses needed to keep up with patient demand
- Improving nurse training and retention are needed to stave off shortages
- The demand for nursing care is driven by Michigan’s older and sicker than average population; public health investments in disease prevention and health promotion are needed to reduce the unsustainable demand for nurses.
Demand for hospital care has surged in Michigan, and, amid this demand, media attention has focused on a critical shortage of nursing professionals. But, amid this growing shortage, many nurses are leaving the field due to stress, burnout, and other factors. Staffing issues have led hospitals to offer recruitment and retention bonuses, while others have unveiled international recruitment strategies.
While this is not a new problem, the demand for nurses has reached a critical juncture. Preventing more severe shortages in the future will certainly require multifaceted strategies to train and retain nursing professionals. Moreover, a successful strategy must also aim to mitigate the population health and demographic factors that drive up demand for nursing care.
Nursing by the Numbers
As of 2018, Michigan had 137,541 licensed nurses – a rate of 13.8 nurses per 1,000 population. This rate exceeded the national average of 12.0 nurses per 1,000 population; however, Michigan has fewer nurses relative to its population than many of its neighboring states (see Map).
Ratio of licensed nurses to population, by state, 2018
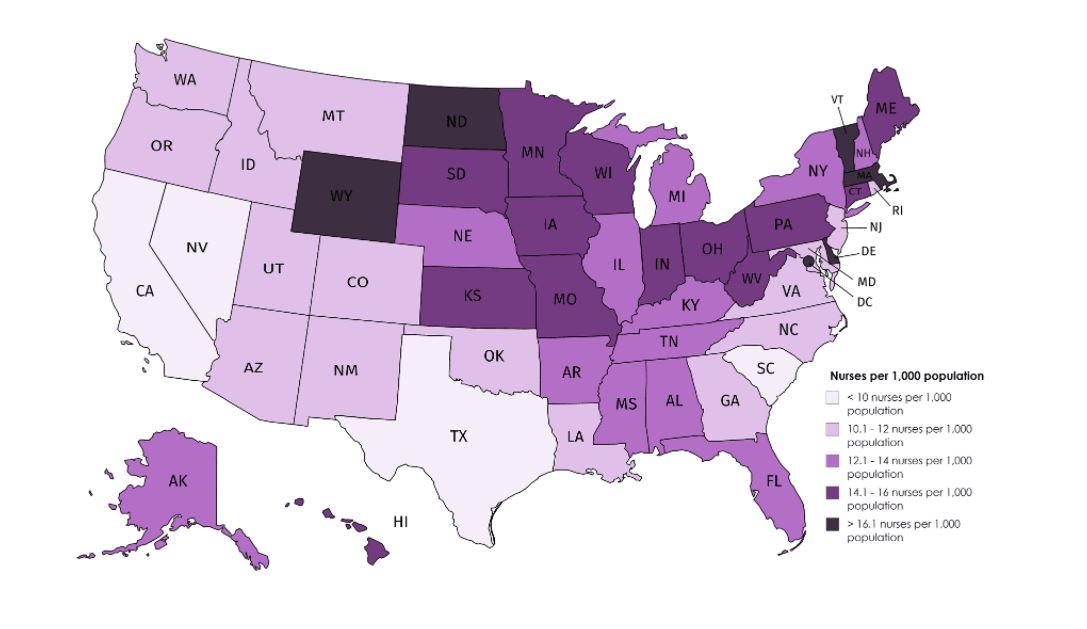
Source: Nurse Journal
While Michigan has an above average proportion of licensed nurses, determining whether this supply is adequate depends upon many factors (such as the health status and demand for nursing services within a population) that can vary tremendously by state and region. Moreover, of all 50 states, Michigan had the highest proportion of licensed nurses not working within the profession (22.2%).
One must also consider the vast differences in roles for licensed practical nurses (LPNs), registered nurses (RNs, with either a 2 or 4-year education), and advanced practice nurses and clinical nurse specialists with post-baccalaureate education and training. Much of the current shortage of nurses appears to be concentrated at the bachelor degree (BSN) level.
Training Nurses
Michigan has long struggled to increase the number of nurses graduating from community colleges and universities; however, the size of each new nursing cohort is constrained by numerous factors.
One constraint is the availability of qualified nursing faculty. Nurses with graduate degrees generally find more lucrative job prospects in clinical practice, care coordination and management, and/or research than in teaching. Availability of nursing faculty thus places limits on the size of nursing school cohorts.
The lack of nursing faculty also limits the capacity to train future nursing educators. According to the American Association of Colleges of Nursing, “8,471 qualified applicants were turned away from master’s programs, and 3,157 qualified applicants were turned away from doctoral programs in 2019.”
To increase the pool of new nurses, governments and other stakeholders could target investments/incentives to bolster the supply of nurse educators (as states like Maryland and Hawaii have begun to do). Strategies might include public funding for supplementary compensation or bonuses, favorable tax incentives, or student loan forgiveness programs.
Retaining Nurses
The escalating demand for new nurses could also be mitigated by employee retention efforts.
According to the 2021 NSI National Health Care Retention and RN Staffing Report:
“[Registered Nurse] turnover increased by 2.8% and currently stands at 18.7%. Since 2016, the average hospital turned over 83% of their RN workforce. In essence, every 6 years, a hospital will have an entirely new RN staff.”
This level of turnover is unsustainable.
While needed reforms could be encouraged through public policy mechanisms, such as licensure and/or Medicare/Medicaid reimbursement rules, many retention efforts might better be handled directly by employers. Given that more than 90 percent of nursing departures are voluntary (i.e., retirements and resignations), there is ample opportunity for hospitals, residential care facilities, and other employers to improve nurse retention.
Conventional retention strategies focused on compensation and other monetary bonuses/incentives may find some success. At the same time, it is important to recognize that money will not solve the underlying feelings of stress, burnout, frustration, and disempowerment that many nurses express.
Long hours contribute to burnout, which accounts for around one-third of all nursing resignations. The long hours forced upon many nurses are strongly associated with patient care errors and dissatisfaction, for which they often bear the blame even when they have no control over scheduling/staffing. Hospitals and other employers of nurses must work to both empower nurses and combat burnout if they are going to successfully reduce turnover and improve employee retention.
Supply vs. Demand: The Value of Prevention
A clogged training pipeline and high rates of job turnover are not the only factors contributing to a nursing shortage – we must also consider factors increasing the demand for nursing care.
As with many things, the Baby-Boomer generation bears much of the blame. As a large segment of the population ages, there is a greater demand for complex care in hospitals and nursing homes. All other factors held constant, an aging population is driving demand for more nurses, especially in states like Michigan where residents over 50 comprise an increasingly substantial proportion of the population.
While age is a principal risk factor for most diseases and disabilities, population health factors and health disparities exacerbate the need for complex and costly nursing care. Among states, Michigan has the eighth highest prevalence of comorbid chronic conditions and among the highest rates of asthma, cancer, hypertension, and mental distress.
In our 2018 report on public health, we spoke extensively about Michigan’s ongoing disinvestment in public health staff and infrastructure. These are the essential governmental services that reduce the risk of disease and injury, keeping people healthy so that they don’t end up in a hospital in need of expensive healthcare services, many of which are delivered by nurses.
Just as the coronavirus pandemic has exposed limits and weaknesses in our health care delivery systems, so too has it highlighted the inadequacy of our collective investment in public health. It is important to address nurse training and retention, but it is even more important for our societal focus to shift to prevention. Without public health investments in disease prevention and health promotion, the demand for nursing will continue its unsustainable growth.
Permission to reprint this blog post in whole or in part is hereby granted, provided that the Citizens Research Council of Michigan is properly cited
