
April 21, 2026
In a Nutshell:
- More than one-third of Michigan residents are obese, and this costly health problem is getting worse.
- Originally developed for diabetes treatment, GLP-1 agonists – such as Ozempic – have been approved for weight management, but the drugs are expensive.
- Michigan policymakers should decide whether the state is going promote wider access to GLP-1 agonists or take a more cautious approach.
One of the recent, highest profile trends in health and weight loss is the use of GLP-1 agonists (e.g., Ozempic, Wegovy, etc.). While the drugs were originally developed for diabetes treatment, their impact on weight loss has been well-documented and several versions have been approved by the U.S. Food and Drug Administration (FDA) for weight management in recent years. These approvals, alongside major media attention and advertising campaigns, have led to a substantial increase in the number prescriptions for these medications.
While the drugs have significant potential in the fight against obesity, GLP-1 agonists are expensive and most private insurers do not provide coverage for their weight loss usage. As a result, access is generally limited to those who can afford the high out-of-pocket costs or low-income residents in states – including Michigan – where Medicaid provides coverage. As public demand for these drugs increases, policymakers should decide whether the state should take an active role in promoting wider access to these drugs as a pathway to better overall public health.
Obesity is a Serious and Growing Health Problem
Obesity is an ever-growing public health problem in the United States and Michigan. Data from the Centers for Disease Control and Prevention estimates that 32.8 percent of the adult population in the United States has obesity, defined as a Body Mass Index (BMI) of 30 or higher. In Michigan, 35.8 percent of the adult population has obesity, which is consistent with the problem being worse in the Midwest than in many other regions.
Figure 1
Adult Obesity Prevalence in the United States, 2023
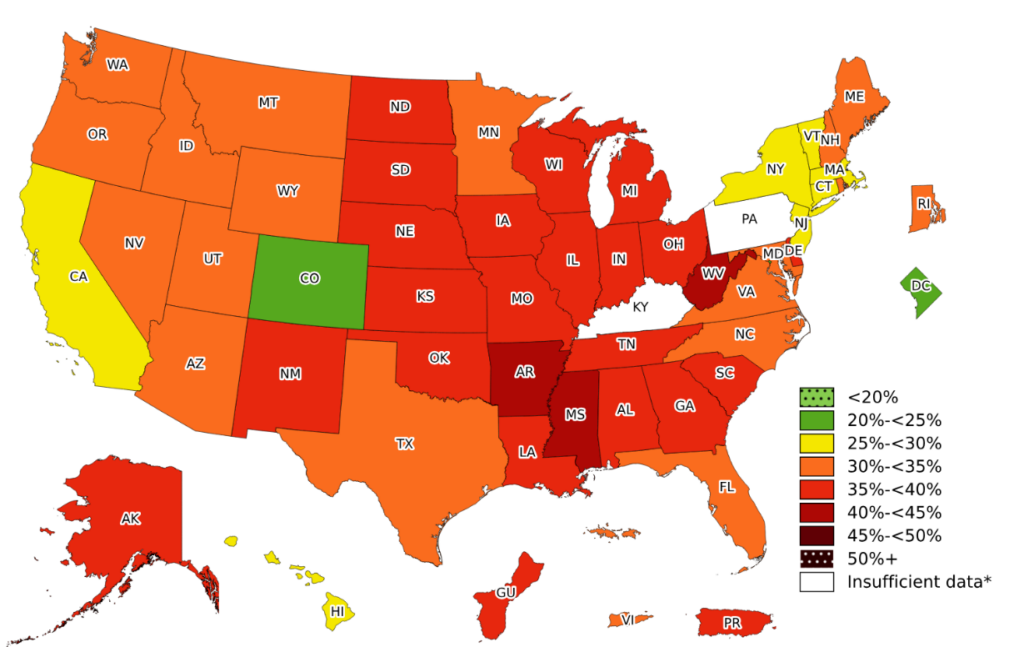
Source: CDC Behavioral Risk Factor Surveillance System, https://www.cdc.gov/obesity/data-and-statistics/adult-obesity-prevalence-maps.html
Obesity rates in the United States and Michigan have been trending upward over the last decade, with a roughly five percentage point increase nationwide and four percentage point increase in Michigan.
Figure 2
Adult Obesity Prevalence in the United States and Michigan, 2011 to 2023
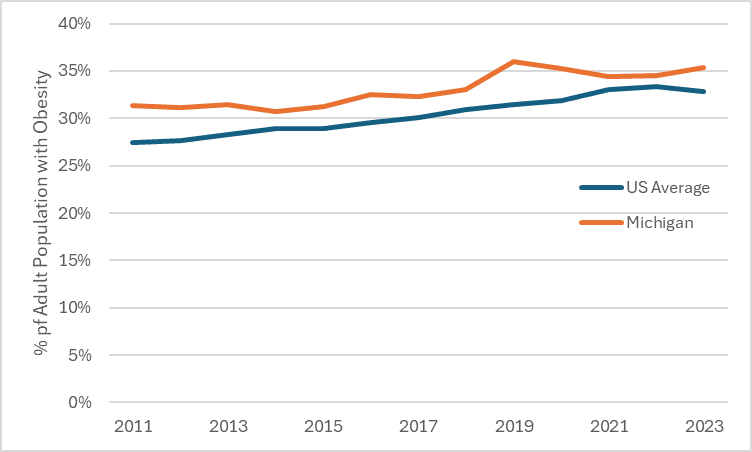
Source: CDC Behavioral Risk Factor Surveillance System, https://nccd.cdc.gov/dnpao_dtm/rdPage.aspx?rdReport=DNPAO_DTM.ExploreByTopic&islClass=OWS&go=GO
While obesity rates are higher in certain populations, obesity impacts every demographic. Obesity rates are higher among women, non-white racial minorities (other than Asians), those with less education, and lower income populations. Obesity is also highest among people between the ages of 45 and 65. That being said, even the demographic groups that have lower obesity prevalence still have reasonably high rates. For instance, 27.1 percent of college graduates – the highest level of education reported in the survey – have obesity compared to 36.5 percent of those who did not complete high school. Similarly, 32.2 percent of White respondents surveyed had obesity compared to 42.0 percent of Black respondents. While children are much less likely to have obesity than adults (~19 percent of people aged 2 to 19), childhood obesity rates have increased to a similar degree as adult obesity rates over the last decade. Many children and adults are also classified as overweight, which consists of a lower BMI than those who are obese but still higher than the recommended range.
Obesity has a major impact on individual health, and subsequentially affects the health care sector and overall economy. Obesity is associated with premature death, high blood pressure, high cholesterol, heart disease, stroke, cancer, Type-2 diabetes, asthma, sleep apnea, osteoarthritis, gallbladder issues, anxiety, and depression. Beyond the health outcomes themselves, research estimates obesity-related medical care costs $170 billion annually in the United States and that lost productivity associated with obesity-related absenteeism alone is between $3.4 billion and $6.4 billion annually.
Obesity is a multi-faceted problem with a variety of causes. According to the CDC, while significant focus is given to the willpower of the individual person, “[m]any factors contribute to obesity like genes, certain medications, poor sleep, gut microbiome, stress, access to affordable food, safe places to be active, and access to health care.” As a result, combating obesity involves many different approaches, including strategies identified by the Research Council in 2014 which could be implemented at the state and local level, as well as in schools.
The Rise of GLP-1 Agonists
One of the most high-profile tools in the effort to decrease obesity prevalence in recent years is a class of medications called GLP-1 agonists. Originally designed to treat Type 2 diabetes, GLP-1 agonists “stimulate the pancreas to release insulin and suppress the release of another hormone called glucagon, both of which help control blood sugar levels in people with type 2 diabetes.” GLP-1 agonists have been utilized for diabetes for the last two decades, but because the drugs also impact the brain, reducing the feeling of hunger and making the user feel fuller longer, many people who use GLP-1 agonists lose weight. This has led the FDA to approve several GLP-1 agonists for weight loss even when diabetes is not present.
GLP-1 agonists have received significant media coverage and celebrity attention, given the major impact these drugs can have on weight loss. Studies have found the use of these drugs can have measurable impacts on weight loss, ranging from five percent to 25 percent body weight loss depending on the conditions. As is the case with most medical interventions, the specific drug, length of utilization, and a host of other factors impact the potential outcomes.
The combination of positive research findings, public attention, and a growing number of approved drugs has led to a massive increase in new prescriptions for GLP-1 agonists in the last few years. Six percent of all adults in one survey reported they were currently taking a GLP-1 agonist and another study showed a 2000 percent increase in new prescriptions for GLP-1 agonists for weight management between 2020 and 2023 (and 2024 figures are likely even higher).
In addition to the direct health benefits, lower heath care utilization, and higher productivity associated with weight loss, other potential benefits of GLP-1 agonists on society include lower spending or demand for groceries and food. The benefits also may not end with weight loss and its consequences. Emerging research suggests GLP-1 agonists might reduce various kinds of addictive behaviors, such as alcohol and drug use, as well as gambling, although much more research is needed on those fronts.
Access to GLP-1 Agonists is Limited
While GLP-1 agonists are not a comprehensive solution to obesity, the approval of GLP-1 agonists as general weight loss drugs has significant potential to improve individual well-being and reduce the societal costs of obesity, meaning that it is likely that broader access and availability of the drugs would have wide ranging benefits. Currently, access to GLP-1 agonists is limited in two related ways.
Shortages
While there has been an explosion in demand for these drugs over the last few years, there has not been a proportionally large increase in supply. Official shortages for several of the leading GLP-1 agonists began in early 2022 and continued until late in 2024. While most GLP-1 agonists have come off the FDA shortage list, it may not mean the drugs are widely available – removing the drug from the shortage list limits the ability of compounding pharmacies to legally produce cheaper, generic alternatives. Leading manufacturers are working to keep up with demand, but availability is likely to remain an issue for some time.
Cost
The cost of GLP-1 agonists is an even larger problem than the shortages. These drugs are expensive, with a typical monthly regimen costing about $1,000. This cost is relevant in two different ways. First, many health insurers do not cover GLP-1 agonists for weight management, meaning that it is extremely costly for many individuals who have been prescribed these drugs to afford them. Further, even for the population that does have coverage that will pay for GLP-1 agonists for weight management, the cost to the insurer (either the government or a private insurer) is very high as a growing number of people are being prescribed these drugs.
The cost problem has led to a variety of responses from governments and insurers around the country. Most notably, Blue Cross Blue Shield of Michigan (BCBSM) announced last year that it would phase out coverage of GLP-1 agonists for weight management by 2025, citing the high costs of the drugs. As part of the announcement, Blue Cross cited data that it was paying $100 million per year in claims for fewer than 10,000 patients to gain access to the medication. In another major announcement, the state employee health plan in North Carolina dropped coverage after forecasting major losses due to spending on GLP-1 agonists. Other employers have followed suit, or opted to not cover these drugs for weight management at all. Most plans on the Affordable Care Act marketplace do not cover GLP-1 agonists for weight management.
Medicaid coverage for GLP-1 agonists varies by state, with Michigan being one of 13 states that provides coverage for GLP-1 agonists for obesity. Michigan has said it does not plan to eliminate this coverage under its Medicaid program, although it has begun to require prior clinical authorization to manage costs. In June, the state reported a monthly cost of around $12 million for these claims, with a more recent analysis showing monthly spending close to $16 million.
Medicare coverage is more complicated. Currently, Medicare cannot cover weight loss drugs, but Medicare’s prescription drug coverage can cover the medication for other approved uses; meaning that those with diabetes or other high cardiovascular risks have access through Medicare. Unsurprisingly, the spending data shows major increases on these drugs over the last few years.
Broadly, this establishes a status quo in which some people who may benefit from GLP-1 agonists are unable to afford them because they do not have coverage for the drug and out-of-pocket costs are high, while others have access to the drug, but the costs associated with those prescriptions are placing significant burdens on public and private insurers. In Michigan, specifically, wealthier people who can pay out of pocket have access to GLP-1 agonists, as well as those who qualify for Medicaid, but people with ordinary incomes and private insurance are largely unable to take advantage of these drugs. In many states, the drugs are only available to those who can pay out of pocket.
Expanding Access vs Taking a Step Back
Many people would like to improve their short- and long-term health but have struggled to find a weight-loss strategy that works. Gaining access to a medication that gives them a leg up on weight loss has the potential to be life-changing. While short-term supply issues exist, the larger problem is the cost of these drugs and the small number of insurers that cover them. Policymakers face difficult questions when it comes to engaging with GLP-1 agonists and weight management, as there is an obvious logic to promoting wider access to these drugs, but creating the right environment for that to occur is challenging. In fact, the status quo is arguably a “worst of all worlds” scenario in which most people do not have access to the drugs, access is conditioned on wealth, and the state’s Medicaid program is on the hook for over $100 million per year in costs associated with GLP-1 agonists.
Policymakers should grapple with whether GLP-1 agonists are something the state wants to promote as a serious tool in the fight against obesity or if they should be seen as a luxury item. Good arguments exist for both approaches, but the state should settle on one and pursue it.
The prevalence of obesity and the magnitude of its costs (individual well-being, medical expenses, economic costs) is a strong argument for pushing to expand access to GLP-1 agonists. If a relatively simple injection can help people live healthier lives and offset wide ranging social costs, it makes sense that the state would want to take action to promote access to these drugs.
The challenge to promoting wider access is the cost of the drugs. Presently, the high cost of the drugs limits who has access in Michigan because most private insurers do not cover GLP-1 agonists for weight management. Private insurers would cover these drugs if they were cost effective to the insurer, but the problem insurers face is that people often change insurance providers when they switch jobs, move to other states, and cycle onto public programs. The incentive to invest heavily in any individual person’s long-term health is lower than if the person was guaranteed to be on their plan in 20 or 30 years. Insurers would happily spend money now to save more money in the future, but individual insurers cannot be sure that their investments will benefit their company specifically over time. It is perfectly understandable why insurers are weary about providing coverage for GLP-1 agonists for weight loss, as the short-term costs are huge, and the long-term benefits might accrue somewhere else.
To solve this problem of insurer incentives and ensure access across the board, the state could mandate private insurers cover these drugs for weight management, similar to the way the state has set minimum coverage requirements for other services. Doing so would either require a large government subsidy or a significant increase in premiums, but it would ensure access and guarantee insurers remain competitive with each other. The state is already providing coverage for these drugs through Medicaid, essentially making a financial investment in this type of treatment and its potential benefits. By ensuring access to these drugs for part of the population while excluding many others who might benefit, the state is making decisions based primarily on ease of implementation – it is administratively easy to provide coverage through Medicaid and more complicated and contentious to enact a law providing coverage for everyone who has private insurance.
Signing on to a policy agenda of promoting GLP-1 agonists means the state would be exposing itself to extremely high costs in the short-term, but the scope of the obesity problem may mean the benefits are worth it. BCBSM reported paying $100 million a year for GLP-1 agonists for weight management, while the state’s Medicaid program is paying even more. Extending this coverage across the board and making the drugs available to anyone with insurance whose doctor prescribed the medication could lead to billions of dollars a year in claims in Michigan alone. Mandating coverage of GLP-1 agonists, funded with tax dollars or increased premiums, without additional work to drive down costs, is equivalent to writing, at a minimum, a nine-figure check every year.
If the state wants to aggressively pursue the long-term payoffs of lower obesity rates by mandating or strongly incentivizing coverage for GLP-1 agonists, part of that means engaging seriously in the work of driving down the cost of these drugs to the extent possible. GLP-1 agonists are cheaper in other countries and much cheaper to manufacture than the current list price in the United States, meaning there is room to drive down prices without driving the drugs from the market. While the federal government certainly has an interest in driving down GLP-1 agonist prices and has more leverage to do so, the state cannot rely on federal action. Previous research by the Research Council has outlined different options for combating prescription drug prices at the state level, some of which could play a role in efforts to address the high cost of GLP-1 agonists.
One option is direct price controls, although that level of regulation may generate undesired economic impacts, such as pharmaceutical companies choosing not to sell these products in the state or shifting costs to other parts of their business to recoup the losses. For this reason, a price control on GLP-1 agonists may not be particularly well-suited for driving down costs, but it could serve as a backstop that limits price increases going forward. Volume-purchase pooling is another potential avenue, as the state could try to drive down the price via bulk purchases across Medicaid and private plans. Additionally, the state could seek out partnerships with other states that offer (or want to offer) Medicaid coverage for GLP-1 agonists for weight management and that might be willing to mandate or promote private insurer coverage for GLP-1 agonists in their states. This partnership of states could present the manufacturers with a willingness to expand the market for these drugs on the condition that the prices come down.
Alternatively, the state may wish to recognize the current GLP-1 agonist situation calls for caution. While the drugs show great promise in clinical trials and celebrity anecdotes, the long-term effectiveness and benefits are unknown. It may be the case that drugs work indefinitely and lead to significant long-term health and economic benefits, but those outcomes are far from certain and it may not be wise to make such a large investment in these drugs this soon. Even stipulating to the positive effects, the size of the impact may not warrant the level of effort and expense contemplated above. If the state does not believe the GLP-1 agonists are worthy of that level of investment at the moment, it may make sense to revisit its commitment to covering the drugs through Medicaid, as spending a lot of money on these drugs through Medicaid and doing nothing to make them accessible to others is not a particularly equitable arrangement.
It is unlikely the market will drive down costs without some push from government in the short term given that the demand for these drugs is well above the current supply and that production is consolidated among a small number of companies. However, on a longer time horizon, it is easy to imagine competition driving prices down low enough that insurers are more willing to cover the drugs and that covering the drugs via Medicaid would become less costly. Similarly, a cautious approach would give policymakers more information about the impact of these drugs on other social costs that would help determine if further action is worthwhile from an overall cost-benefit perspective.
No easy answer exists for policymakers, but they should engage with the issue now given the massive increase in GLP-1 agonist usage. If the state is serious about pursuing wider adoption of these drugs given the benefits, part of that approach should be active measures to attempt to drive down costs. But if policymakers are not yet convinced that expanding access is the right course, it does not make much sense to spend hundreds of millions of dollars on these drugs for only the Medicaid-eligible population.
Conclusion
Obesity is a major public health problem in the United States and Michigan that continues to get worse. Over the last few years, GLP-1 agonists have garnered positive research findings, public attention, and more FDA-approvals, leading to a massive increase in new prescriptions for weight management.
GLP-1 agonists remain inaccessible to most people, as they are expensive and not covered by most insurers. Public and private insurers that do cover GLP-1 agonists for weight management are facing significant budgetary impacts given the costs of the drugs.
Policymakers should grapple with whether GLP-1 agonists are something the state wants to promote as a serious tool in the fight against obesity or if they should be seen as a luxury item. Good arguments exist for both approaches, but the state should settle on one and pursue it.
