
March 25, 2025
In a Nutshell:
- More than 70 percent of Michigan’s citizens are fully vaccinated against COVID-19
- Vaccine uptake remains low in some communities, and the unvaccinated are driving the current surge that threatens to overwhelm hospital capacity
- The communities that have eschewed the COVID-19 vaccine are characterized by lower health literacy and a history of poor health behaviors and outcomes.
While Michigan has passed the 70 percent mark for the number of residents vaccinated against COVID-19 (a now arbitrary threshold in the face of highly transmissible viral variants), pockets of the state remain where just a third of residents have completed their vaccination. As a result, the safe, effective, and widely-available vaccines have not been the magic bullet to end the pandemic some had hoped for. The consequence: Michigan’s hospitals are now strained for capacity due to hospitalizations driven by the unvaccinated.
What accounts for this resistance to life-saving preventative health measures?
Some have attributed differences in community vaccination rates to differences in education level (indeed, more educated communities tend to have higher vaccination rates). Others have pointed to politics (an NPR analysis found that counties that supported former President Trump have both lower vaccination rates and greater morbidity and mortality from COVID-19). While politicization of public health continues to be problematic, vaccination trends aren’t solely attributable to politics (almost 60 percent of residents in conservative Livingston county are fully vaccinated against COVID-19, while coverage in Detroit is just 36 percent).
Differences in COVID-19 vaccination rate by Michigan county
A deeper examination of data reveals that counties with healthier environments (including environmental conditions such as air pollution and drinking water violations, but also housing, transportation, unemployment, poverty income inequality, educational attainment, availability of health providers, and health insurance coverage) have much higher rates of vaccine uptake. These counties also tend to have healthier behaviors. Conversely, counties that are already unhealthy (those with lower preventative health utilization and higher rates of unhealthy behaviors) are least likely to utilize the vaccine.
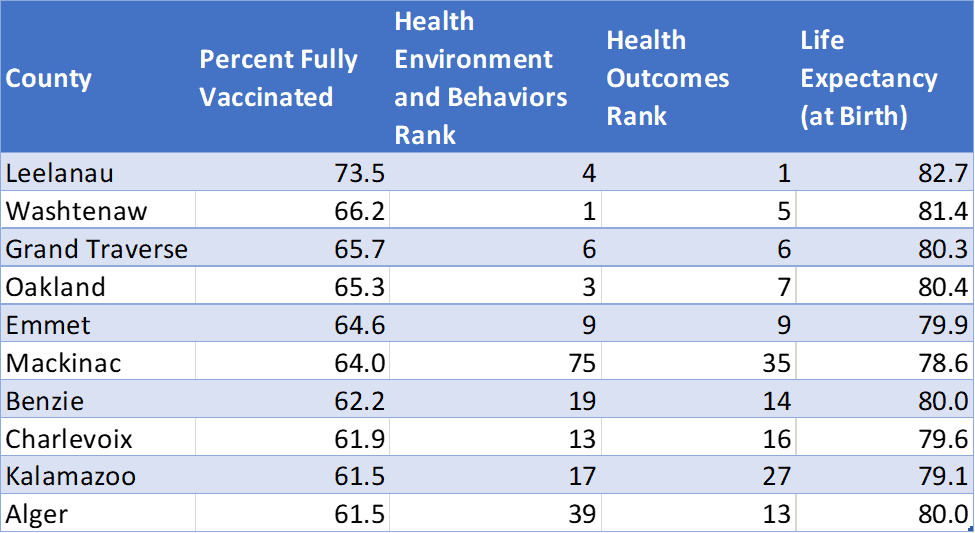
The ten counties with the highest vaccination rate are also generally rated high for their health environment and health outcomes. Additionally, all ten of these counties have a life expectancy above the state average (78.1 years).
Michigan Counties with the Highest Rate of COVID-19 Vaccination
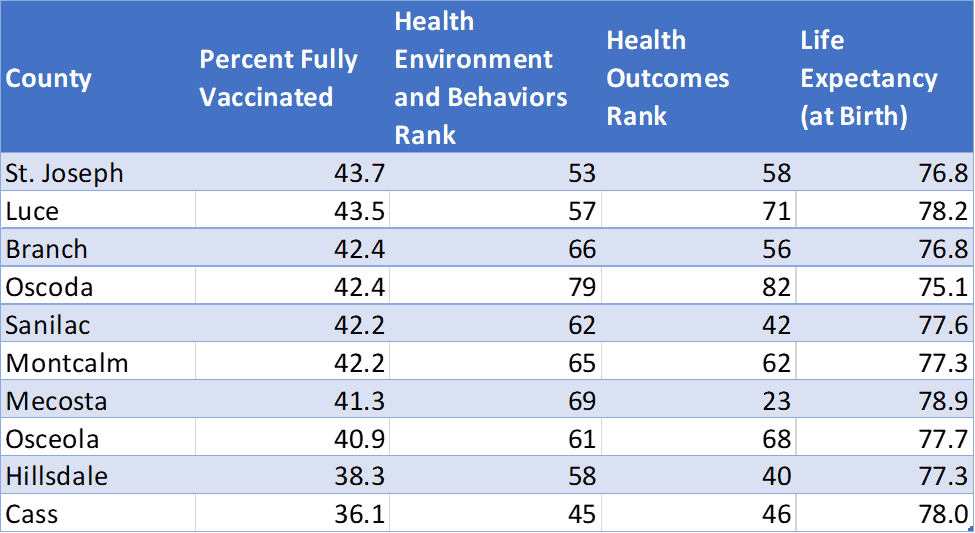
Conversely, the counties with the lowest proportion of fully vaccinated residents rank low on overall health. Most also have a below average life expectancy.
Michigan Counties with the Lowest Rate of COVID-19 Vaccination
Unfortunately, these differences in vaccination rates further contribute to the larger health disparities that exist among different communities. These data also suggest that differences in health literacy contribute to differences in health behaviors and, ultimately, health outcomes throughout Michigan.
Vaccine hesitancy
As I’ve previously written, vaccine hesitancy continues to threaten public health.
Mixed signals from public officials combined with decades of growing mistrust in government have hindered the coronavirus response throughout the U.S. The dark side of Americans’ rugged individualism is that it has eroded confidence in social, political, and scientific institutions, and even in the very concept of expertise. Thus, our greatest challenges in the ongoing pandemic have turned out to be social and political rather than logistical or scientific, and vaccine hesitancy has emerged as a leading barrier to administering vaccines to protect against COVID-19.
While substantial resources are expended on making biomedical advances, these advances are of little value if people resist or refuse them. The public therefore has a collective interest in sharing the message that vaccines are safe, beneficial, cost-effective, and necessary. More attention must be placed at the intersection of public health, marketing, and education to identify more effective strategies for engaging the general populace in public health efforts, particularly when it comes to preventative measures and/or health-enhancing behavioral changes.
If facts and truth hold less persuasive power than beliefs and values, policy efforts must necessarily concentrate on the latter. Addressing individual and community anti-vaccine attitudes holds the greatest potential to increase the state’s vaccination rate, but given the prevalence of anti-vaccine sentiment, this will not be easy. Vaccine hesitancy has long affected childhood immunization rates in Michigan, and has left the state below average with regard to the annual flu shot. It is therefore not surprising to see widespread hesitance toward the new coronavirus vaccines.
Michigan’s urban/rural (and suburban) divide creates unique challenges to immunization efforts, meaning there’s no one-size-fits-all solution. Vaccine hesitancy is best understood as a broad spectrum of apprehensions and/or beliefs. The source(s) of hesitance in Escanaba, Alpena, or Clare is likely to be quite different from the source(s) of hesitance in Detroit; likewise, neighbors in any of those cities may have different fears about the vaccine and reasons for not yet getting it. Multifaceted efforts are needed to counter misinformation and ease vaccine concerns or doubts.
As this wave of COVID-19 overlaps with flu season, the influenza vaccine warrants consideration. In a previous blog, I highlighted the fact that a majority of Michiganders also skip their seasonal flu shot, even though influenza is a substantial source of morbidity and mortality. Leading into the pandemic, more than half of the population continued to avoid or neglect the seasonal flu vaccine each year.
Michigan’s rate of flu vaccine utilization falls below the national average for both children and adults. Some Michigan counties—particularly those with large proportions of low-income and/or rural residents—have especially low rates. There are also longstanding racial disparities in influenza vaccination. It is especially important to address these differences in flu vaccine utilization since severe influenza (requiring hospitalization) is more prevalent in lower-income communities that already suffer from poorer health overall.
Vaccine hesitancy creates risks and costs for every person in Michigan, including increased health care spending and diminished productivity because of missed work or school—to say nothing of avoidable hospitalizations and premature deaths. Policies that remove barriers to vaccination and increase the number of people utilizing vaccines and other preventative health services should therefore be encouraged.
Investing in health literacy and health education
The same dangers of politicization and misinformation that have surrounded the use of masks and other face coverings are applicable to all public health interventions and/or recommendations—including vaccinations. Mixed signals from public officials combined with decades of growing mistrust in government have hindered the coronavirus response throughout the U.S. Similarly, political posturing around any forthcoming vaccines will benefit no one.
Nonetheless, government has a crucial role to play when it comes to vaccines, promoting research and development, ensuring safety and efficacy, facilitating the logistics of supply and distribution, and addressing barriers that may stand between citizens and valuable public health measures (such as issues of cost and access). It should be clear to all that the government’s role in public health, therefore, is one of policy, not of politics.
