
July 28, 2026
In a Nutshell:
- Shortages of behavioral health providers (from psychiatrists to counselors) have limited access to treatment for mental health and substance use disorders.
- As demand for behavioral health services increases, Michigan must address recruitment and retention of the behavioral health workforce to prevent more severe shortages in the long run.
- Strategies to ensure an adequate supply of behavioral health providers range from loan repayment and increased reimbursement to modification of scope of practice and licensure laws to investment in public health screening and prevention of behavioral health disorders.
In August of 2020, I cautioned that Michigan was falling short on mental health services. While this problem is now widely acknowledged in Lansing, incremental policy changes have been insufficient to address the magnitude of the problem.
While addressing the behavioral health needs of Michigan’s population requires complex, multifaceted policy solutions (as discussed in our report published last year: Meeting the Mental Health Needs of Michigan Youth with School-Based Health Services), a key focus of public health policy must be to ensure an adequate supply of behavioral health care providers.
Moreover, because workforce development issues unfold over time, swift action is required to avoid worsening of existing shortages over time.
Behavioral Health Providers: Supply and Demand
According to an analysis from the University of Wisconsin Population Health Institute, Michigan has approximately one behavioral health provider for every 360 citizens. There is, however, wide variation in the supply of behavioral health providers at the county level. Only 15 of Michigan’s 83 counties have ratios below this statewide average, leaving 68 counties with scarcities to varying degrees. Those 15 counties are mostly the urban counties with higher population densities.
Behavioral Health Providers in Michigan by County, 2019
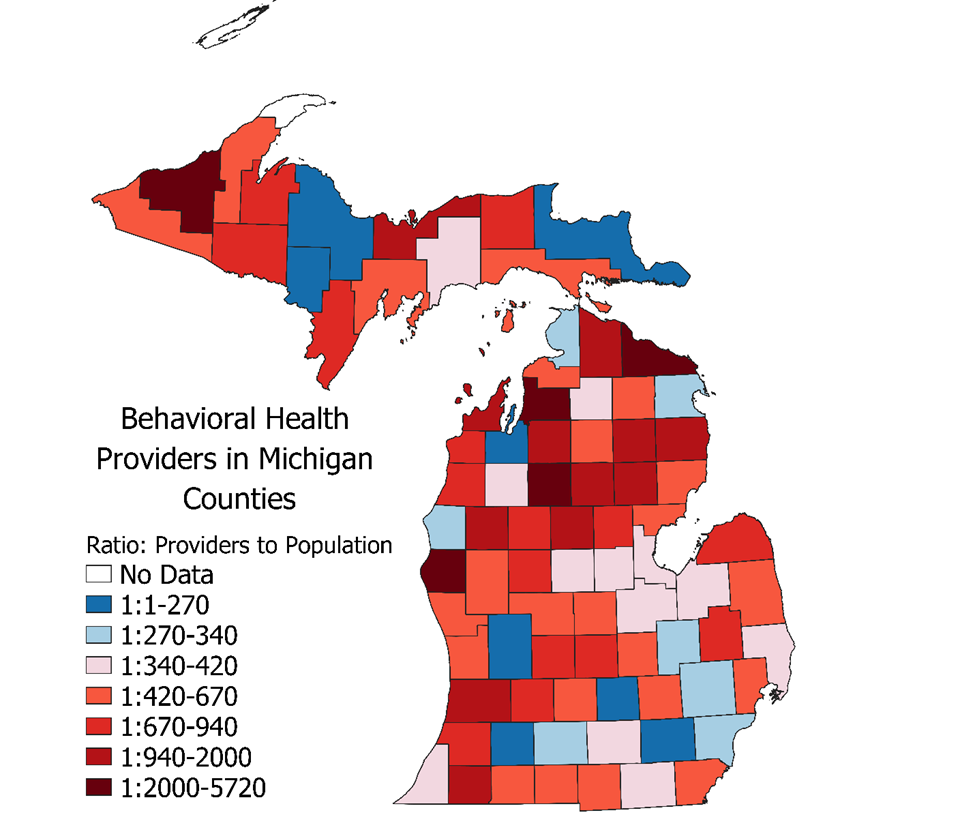
In part because of this wide variation, Health Professional Shortage Areas (HPSAs) for mental health professionals are spread throughout Michigan and are particularly concentrated in rural areas. A HPSA denotes a shortage of primary, dental, or mental health care providers as designated by the federal Health Resources & Services Administration (HRSA) based upon the ratio of practicing health care providers to area population relative to standard estimates of adequate (not optimal) provider density. Health Professional Shortage Areas can be geographic areas, populations, or facilities, such as a correctional facility or state mental hospital.
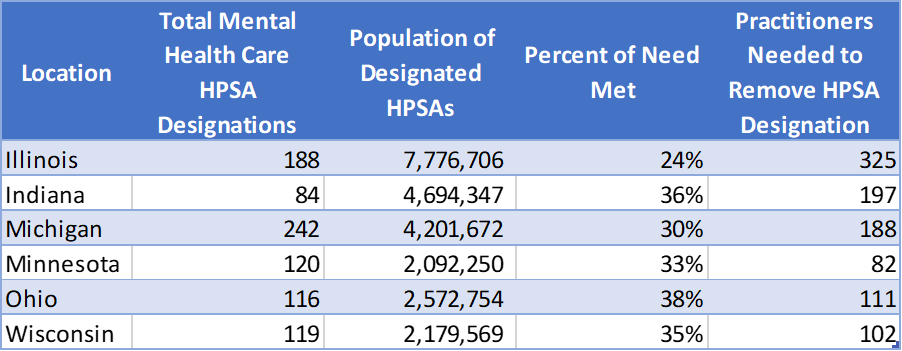
Michigan has a total of 242 designated HPSAs for mental health care. This places more than 40 percent of the state’s population (4.2 million people) in a HPSA with unmet behavioral health care needs. It would take an additional 188 FTE advanced providers distributed throughout shortage areas to remove these HPSA designations.
Mental Health Care Health Professional Shortage Areas (HPSAs) in Michigan, as of September 30, 2021
It is important to note that the HPSA designation is used to prioritize the distribution of funds and services intended to bolster health care infrastructure in severe shortage areas – elimination of HPSA designation eligibility would not necessarily indicate a completely adequate supply of providers.
Even in areas of Michigan without HPSA designation, numerous barriers (including an inadequate supply of providers) prevent access to behavioral health treatment for those who need it. Nearly 40 percent of Michiganders with a behavioral health condition go without treatment, and for those with substance use disorders, 80 percent do not receive care.
Estimating exactly how many more behavioral health providers Michigan needs is a difficult task for several reasons. Accurate data are needed to both assess current provider capacity and population need for behavioral health care services. Unfortunately, Michigan lags in its investment in public health, hampering data collection, surveillance, and analysis due to needs for both personnel and modernized information systems. Overlap in scope of practice between different types of behavioral health care providers adds complexity to any estimate.
According to the best available estimates from the Health Resources & Services Administration (HRSA), Michigan already has large shortages that will persist through the next decade.
Behavioral Health Care Provider Supply and Demand in Michigan by Provider Type, 2016 and 2030
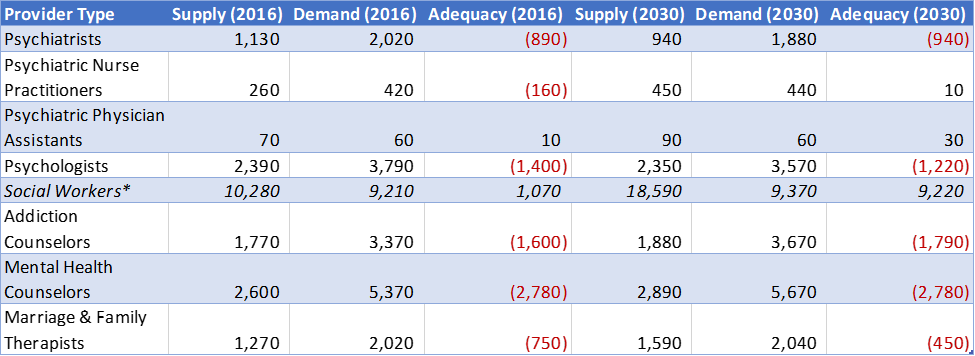
*Due to data limitations, this includes all social workers trained at the master’s level or higher, not just those focusing on clinical mental health or substance abuse. Consequently, the supply of social workers is overstated in these data.
While Michigan may expect to see growth among some provider groups (e.g., psychiatric nurse practitioners), this shouldn’t be construed as cause for optimism (particularly, in the case of NPs and PAs, amid a corresponding decrease in the number of psychiatrists).
These estimates must also be understood in the context of their modeling in 2019. The supply estimates do not adequately account for accelerated rates of attrition and burn-out among providers observed during the COVID-19 pandemic. Additionally, because of the rapidly increasing prevalence of behavioral health conditions in Michigan (and throughout the U.S.), these estimates likely understate demand for care in 2030. Moreover, because demand was modeled on historical population characteristics and health care utilization and treatment patterns (wherein more than a third of those needing treatment in Michigan did not get it), the above estimates may, in fact, be a gross understatement of future behavioral health workforce shortages.

Addressing Michigan’s Behavioral Health Workforce Pipeline
There is no single policy solution that will solve long-term shortages of behavioral health providers. Rather, efforts must be made to address all aspects of workforce development (from education/training and recruitment to employee retention strategies and service delivery improvements). These efforts must be rooted in evidence-based planning, which means improvements in capacity for data collection and analysis.
There are a wide range of potential recruitment and retention strategies for the behavioral health workforce, some of which are already in place. For instance, I suggested previously that the state might consider expanding loan repayment options. The current loan repayment program for HPSAs turns away nearly half of applicants due to insufficient funding. Adequately funding the current state loan repayment program should be an obvious policy priority, however expanding loan repayment options for other provider types or for certain providers practicing outside HPSAs might be considered. While loan repayment programs are useful retention tools for graduate-level providers practicing in the state, undergraduate scholarship opportunities for behavioral health disciplines might be coupled with recruitment efforts at the college, high school, or even middle school level.
The state’s Medicaid Expansion dramatically increased the number of people with coverage for behavioral health care; however, low Medicaid reimbursement rates for behavioral health care limits provider availability. Increased Medicaid reimbursement would not only remove barriers to treatment for Medicaid-eligible individuals but would also bolster funding to retain behavioral health providers, particularly in lower-income rural and urban areas.
Addressing service delivery is essential both for ensuring that available providers are deployed efficiently and effectively, and for making sure educational requirements and training prepare future providers to operate within new care delivery models. Plans for care integration of behavioral health and primary health care are essential, including service models that integrate behavioral health specialists as consultants in general medical care. Michiganders will also be better served by a behavioral health care workforce equipped to serve individuals with co-occurring mental health and substance use disorders.
Reforms to scope of practice may also facilitate improved treatment options. Psychiatric nurse practitioners are increasingly essential to address behavioral health care needs—especially in areas with low concentrations of psychiatrists. This is particularly true when nurse practitioners are authorized to work to the full extent of their training and education. While licensed behavioral health professionals are generally educated at the master’s degree level or higher, Michigan might consider creating limited opportunities for bachelor’s prepared providers paired with support for completion of a terminal degree.
Lastly, strategies should not focus solely on the supply of providers, but also the demand for services. Setting aside aforementioned barriers to care, the individual-level focus of behavioral health care must be combined with the group/community/population-level focus of public health for optimal public benefit. For instance, one-on-one psychosocial counseling does not address the needs of people for whom levels of psychological distress do not meet a baseline diagnostic threshold, missing the opportunity for early intervention and prevention. In contrast, a public health approach to behavioral health can “address the needs of the total population, including at-risk subgroups, through multiple levels of intervention and to promote the public’s behavioral health and psychological well-being.”
The need for increased and improved behavioral health services in Michigan is well-documented, and numerous organizations (Citizens Research Council included) have proposed viable solutions to meet this need. Moreover, with a rebounding economy and infusion of federal dollars, the state has found itself with an unprecedented amount of discretionary resources. The only thing standing between Michigan’s citizens and better behavioral health services is the political will to act.
