
July 28, 2026
In a Nutshell:
- Michigan has a shortage of primary care providers, and the situation is projected to get worse in the coming years.
- Many states have expanded the scope of practice for nurse practitioners as one way to address the provider shortage, but Michigan has not.
- Expansion of nurse practitioner scope of practice is generally opposed based on the belief it will lead to substandard and/or costlier care, but studies generally show patient outcomes do not suffer in states with expanded nurse practitioner authority and the data on cost impact is incomplete.
Michigan has a shortage of health professionals across the board, but there is a particular need for primary care providers (PCP). Currently, there are 288 Health Professional Shortage Areas (HPSAs) for primary care spread across the state, with acute shortages concentrated in the northern half of the Lower Peninsula. Shortages are less prevalent in more populated counties. Further, it is projected that the state will be short by 800 primary care doctors by 2030. Lack of access to primary care comes with a host of potential problems due to delays in care that can lead to worse health outcomes and higher treatment costs.
The overall shortage and malapportionment of PCPs in Michigan has been an area of concern for many years and resolving it is challenging because the reasons for the shortages are complex and multifaceted. For instance, many of those who have invested significant time and resources into the training required to become a doctor don’t pursue work as a primary care doctor but instead choose more lucrative specialties. Earlier retirement ages and an aging general population are also contributing to the growing discrepancy between the supply of providers and the demand for medical services.
Policy solutions should be centered around addressing the causes of the shortages to the extent possible, but other options should be on the table to meet the ultimate goal of ensuring the delivery of cost-effective health care to the state’s residents. Policy options fall into several different categories: increasing the supply of doctors, allowing doctors to deliver services more efficiently, and expanding the services that can be performed by other health professionals.
Several specific policy strategies have been proposed, and in some cases implemented, to address the PCP shortage through the lens of increasing the supply of doctors and improving the efficiency with which doctors can practice. These initiatives include increased funding for more residency slots in hospitals with higher needs, student loan forgiveness programs, and expanding the use of technology and telehealth services when delivering care. Many states, including Michigan, have taken various measures to implement some of these strategies, but federal initiatives are likely necessary to carry out some of the larger and more expensive efforts, such as expanded residency slots and loan forgiveness.
Scope of practice, which refers to the range of activities each type of health professional is permitted to perform in the state, is one option that fits squarely within the arena of state policy. Many other states have less restrictive scopes of practice for non-physician health professionals, particularly nurse practitioners. Reducing the restrictions on nurse practitioner scope of practice in Michigan has been raised as a potential solution to the PCP shortage, but the state has not acted on these proposals.
As the state looks ahead to a variety of health care provider shortages in the coming years, it should revisit the discussion about broadening the scope of practice for nurse practitioners as part of its overall efforts to ensure access to care in Michigan.
Scope of Practice Laws
Scope of practice laws determine what types of services health professionals can provide and under what circumstances. These laws exist primarily to protect patients from receiving poor care from health care professionals who may not have the skills or training necessary for the treatment the patient requires. While many doctors and organizations that represent them – such as the American Medical Association (AMA) – stand firmly behind restrictive scope of practice laws, others argue that the restrictions on certain qualified health care professionals are harmful to patients who could benefit from their services.
In response to the growing health care professional shortage, many states have expanded their scope of practice laws, often expanding autonomy for nurse practitioners, in particular. Nurse practitioners are a type of Advanced Practice Registered Nurse (APRN) – licensed nurses who provide primary and/or secondary medical care in ambulatory, acute, and long-term care settings. APRNs receive post-graduate education and training and a master’s or doctoral degree, along with national board certification, is required for entry-level practice.
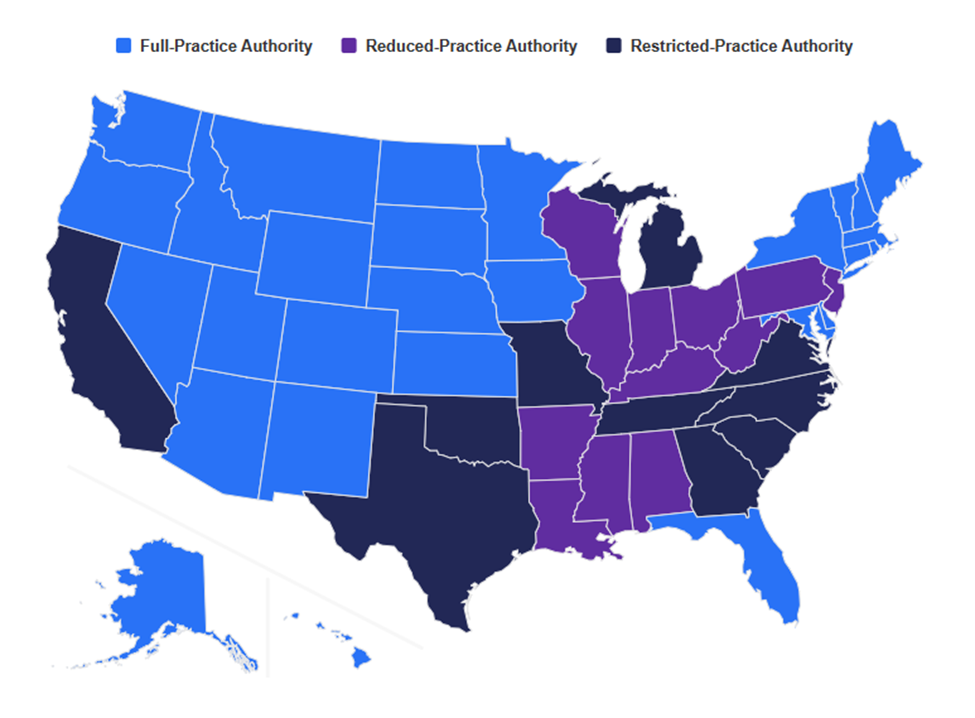
About half of the states allow “full practice” authority for nurse practitioners while the other half enforce reduced or restricted practice.
- Full Practice: Nurse practitioners can perform the full scope of practice without a supervising or collaborating physician. Scope of practice includes diagnosing patients, ordering tests, prescribing medication, and operating their own independent practices. Some states require additional supervised experience or training before allowing full practice authority.
- Reduced Practice: Nurse practitioners can perform some activities without physician supervision. These states generally restrict nurse practitioners from operating their own practices or prescribing certain types of medication.
- Restricted Practice: Nurse practitioners must work under the supervision of a physician for their entire scope of practice.
Nurse Practitioner Scope of Practice by State
Source: Nurse Journal https://nursejournal.org/nurse-practitioner/np-practice-authority-by-state/
Nurse Practitioner Scope of Practice Laws in Michigan
Michigan’s scope of practice laws are considered to be relatively restrictive. Michigan has several laws and policies that work together to restrict the scope of practice for different health professionals, including nurse practitioners. Unlike most other states, nurse practitioners in Michigan are not explicitly identified as PCPs in law or policy.
While Section 172 of the Public Health Code permits the Board of Nursing to issue specialty certifications to registered nurses with advanced training, who are licensed and meet national certification requirements as a nurse midwife, nurse anesthetist, or nurse practitioner, APRNs are still required to practice under the supervision and delegation of a physician (referred to as a “collaborative agreement”). In addition, Michigan law requires a collaborative agreement in order to be reimbursed by the state Medicaid program. ARPNs in Michigan may prescribe certain drugs without the delegation of a physician.
Further, Michigan APRNs are restricted from forming independent practices. The Michigan Limited Liability Company Act only allows members of a “learned profession,” such as a physician, surgeon, or attorney to form a limited liability company or professional services corporation. Therefore, APRNs must either practice under the business license of a physician or hire a physician collaborator to own and operate an independent practice.
Michigan law was amended to expand scope of practice for pharmacists, but not for nurse practitioners. The expansion for pharmacists, which included authorizing pharmacists to order and administer vaccines and laboratory tests, was largely a response to the high demand of the COVID-19 Pandemic. During the pandemic, the “test and treat” program was operated at 66 pharmacies to provide access to COVID-19 testing and treatment for individuals experiencing mild to moderate symptoms who were at high risk for more severe disease. The scope of practice expansion for pharmacists provided cost-effective access to common immunizations and tests that could continue to be beneficial for the general public.
Proposed legislation to expand the scope of practice for nurse practitioners was introduced in 2023 as a response to the lack of care in rural populations, in particular. Like the policy change for pharmacists, the legislation would expand the scope of practice for certain nurse practitioners who met a long list of requirements, which includes graduate-level courses and national certification, and allow the Board of Nursing to set any additional requirements.
Balancing the Costs and Benefits of Expanded Scope of Practice
While it appears that expanding the scope of practice for nurse practitioners in Michigan to the levels enjoyed by nurse practitioners in many other states would be a straightforward step toward solving Michigan’s current and future shortage of primary care providers, there are a number of concerns about the impact of doing so.
A key source of concern is that doctors receive much more training than other health professionals (between 12,000 – 16,000 hours for doctors and 500 – 720 hours for nurse practitioners). As a result, nurse practitioners do not have the same clinical experience, training, and education as doctors, and could put the health of the public at risk by allowing them to provide the services of a primary care doctor.
While it is true that doctors and nurse practitioners receive different training and carry different experiences, policymakers do not need to consider whether nurse practitioners are the same as doctors. The public policy question is whether nurse practitioners operating under a broader scope of practice would provide safe and effective primary care that would be a net benefit to the state.
An increase in medical costs because nurse practitioners tend to order more tests and prescribe certain medications more frequently is one potential negative impact that could arise from expanding nurse practitioner scope of practice. According to data from the AMA, nurse practitioners:
- Ordered more than four times as many X-rays as doctors
- Required twice as many biopsies to diagnose cancer as doctors
- Were 15 percent more likely to prescribe antibiotics than doctors
- Prescribed opioids to more than half of their patients at a higher rate than doctors (6.3 percent to 1.3 percent)
Data shows removing the physician supervision requirements may result in increased utilization of patient referrals to medical doctors.
While there is some research that shows most individuals prefer physicians over nurse practitioners, there is little evidence to show that receiving care from a nurse practitioner leads to poorer quality of care. In fact, several studies, including randomized controlled trials, have shown that the quality of care delivered by nurse practitioners is equal to or better than physician-delivered care in similar settings. A systematic review of the relationship between state-level nurse practitioner scope of practice policy and access to care found that utilization of primary care services was greater in states with less restrictive policies. However, there was mixed evidence as to the impact on whether nurse practitioners improve care of underserved populations, and the impact on patient satisfaction.
In other words, expanding scope of practice for nurse practitioners demonstrates some positive results regarding access to care, but the policy has not been shown to be universally beneficial across multiple categories. However, no studies found that nurse practitioners provide substantially worse care or lead to significantly poorer health outcomes. While people may continue to prefer physicians, there is little evidence to show that only physicians can effectively handle the services of a PCP.
Essentially, the potential negative impacts of expanding nurse practitioner scope of practice boil down to the idea that nurse practitioners are only able to achieve similar outcomes to doctors by running more tests and making more referrals than doctors, which is costly and unnecessary.
In the case of an increase in referrals, there is not a clear explanation for the increase. The reason could be that nurse practitioners are less capable than doctors and therefore need to refer more cases to doctors when they are not being directly supervised by one. These referrals are costly, but the available data does not assess the associated costs of supervision compared to referrals. Even if it is the case that nurse practitioners are making up for their lack of training and expertise with more referrals and tests, it is not clear that this would be a net negative. Certainly, if the state were to expand the scope of practice for nurse practitioners, it could institute a study to determine whether this referral increase occurred in Michigan and whether it was due to nurse practitioners’ limitations, or other factors such as resources, liability fears, or patient complexity. But the simple presence of more tests or referrals is not a reason to oppose expanding nurse practitioner scope of practice.
The overall question the state needs to ask is whether expanding the scope of practice for nurse practitioners would improve primary care compared to the status quo – not compared to an ideal. The evidence suggests that patient outcomes would not suffer, and there is at least some section of the population that would be willing to see a nurse practitioner even if a doctor was available at a similar cost.
Given that there is a shortage of primary care providers, adding more empowered nurse practitioners to the mix – particularly with the kinds of enhanced qualifications proposed by many advocates – seems to make sense as part of an overall effort to improve access to care. This approach is not guaranteed to solve the problem, particularly in the worst shortage areas, but every little bit helps. At the very least, the state should take the question seriously and attempt to directly study the potential cost increases that could be associated with this change, as the state’s job is to balance the costs and benefits, not merely avoid costs.
Conclusion
Michigan has a shortage of primary care providers and the situation is projected to get worse over the next decade. Solving this problem will require a variety of different solutions, many of which will include action at the federal level. One of the key state-level options available to Michigan is expanding the scope of practice for nurse practitioners, as many other states have done.
In the context of a provider shortage, the state’s focus should be on providing quality care. Nurse practitioners in expanded practice states appear to do so. Policymakers need a more detailed and accurate understanding of the financial costs of expanding the scope of practice for nurse practitioners, especially when it comes to increased utilization of tests and referrals. More importantly, however, that cost needs to be weighed against the significant toll the primary care provider shortage has on the public health and financial wellbeing of the state.
