
March 25, 2025
In Summary:
- The State of Michigan’s new “Vacc to Normal” plan ties the termination of public health orders/restrictions to various vaccination thresholds.
- While many people crave a sense of normalcy, our experience with COVID-19 exposed various political, social, and economic deficiencies in our pre-pandemic normal.
- Using this past year of humbling lessons to make systemic policy changes will help us do better than “Vacc to Normal” and refocus public policies to take us “Vacc to the Future.”
The coronavirus pandemic has upended life for many Americans for over a year (and counting) and continues to rage around the globe. A common mantra throughout the tumult has been the desire to go back to normal. A longing for some comforting sense of normalcy is natural and expected, and yet the economic, social, and political problems laid bare by COVID-19—an underfunded and underdeveloped public health workforce and infrastructure, an outdated and ineffective social safety net, an escalating youth mental health crisis, and glaring health disparities and social inequities, to name just a few—might cause some to question if going back normal is really an adequate goal.
Moreover, as emerging pandemic diseases are increasingly poised to become the new normal, any public sense of normalcy may ultimately be contingent on local, national, and global public health reforms and innovations. It is also becoming increasingly apparent that whatever normal we eventually settle upon, it will likely be a normal in which SARS-CoV-2 remains an endemic virus causing future reinfections.
Increasing vaccine uptake is certainly one important mechanism for restoring a sense of normalcy, but widespread vaccine hesitancy is undermining vaccination efforts.
Governor proposes moving things “Vacc to Normal” in Michigan
Last week, Governor Whitmer proposed a “pathway to return to normal.” This “Vacc to Normal” challenge ties the rescindment of pandemic-related public health orders (e.g., capacity restrictions and gathering limitations) to four vaccination-based targets.
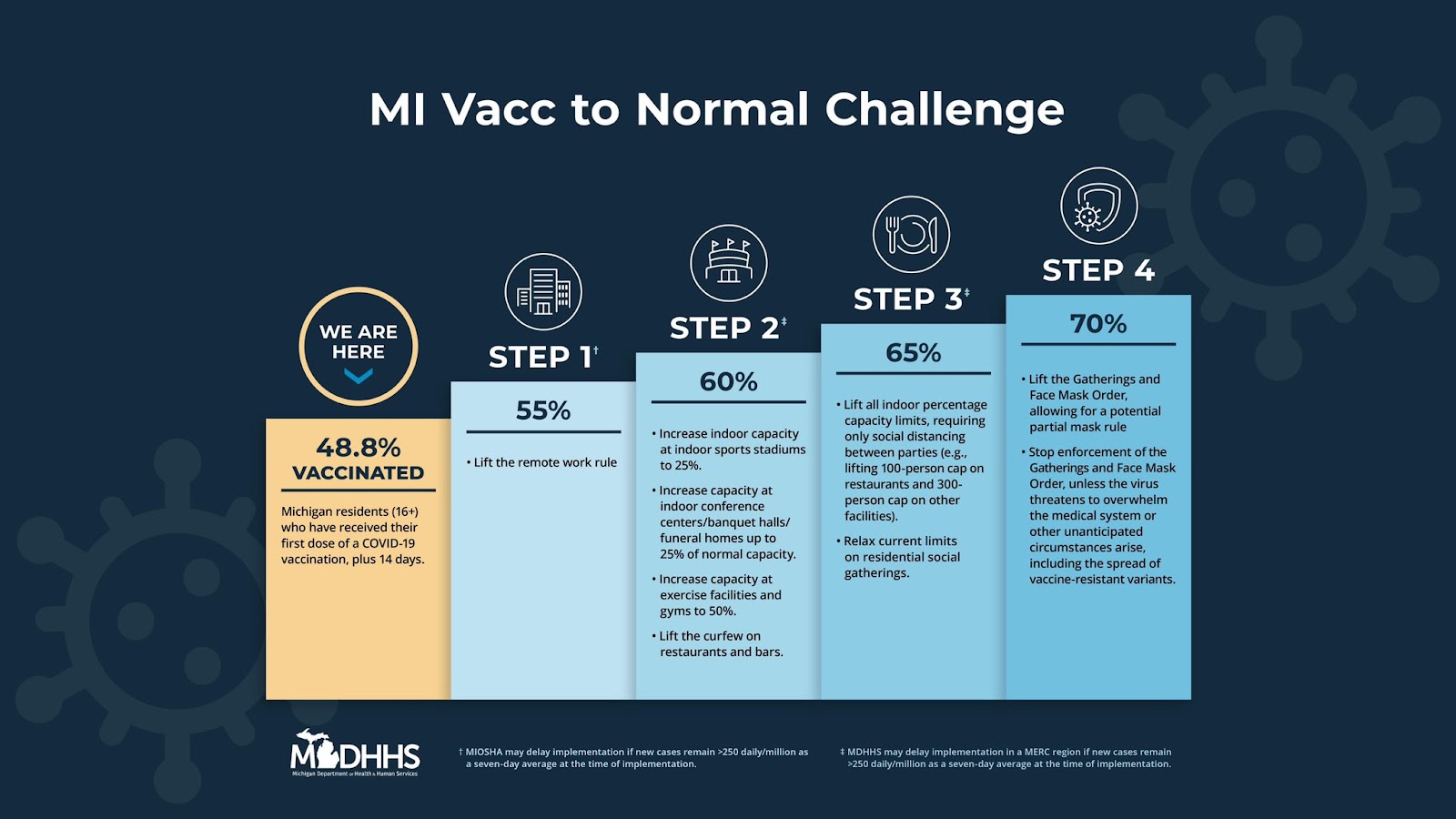
The fourth such milestone is for 70 percent of eligible Michigan residents to receive at least one dose of any vaccine (despite the two most prevalent vaccines—Pfizer-BioNTech and Moderna—requiring two doses to confer optimal immunity). After reaching this milestone, the state will lift the public health order limiting gatherings and requiring face masks (subject to certain caveats).
The White House has set a similar target of administering at least one dose of vaccine to 70 percent of the U.S. population by July 4th, but the 70 percent target for vaccines in arms may take a while longer to achieve in Michigan, given the state’s chronic struggle with low immunization rates.
A Fly in the Ointment: Vaccine Hesitancy
Mixed signals from public officials combined with decades of growing mistrust in government have hindered the coronavirus response throughout the U.S. The dark side of Americans’ rugged individualism is that it has eroded confidence in social, political, and scientific institutions, and even in the very concept of expertise. Thus, our greatest challenges in the ongoing pandemic have turned out to be social and political rather than logistical or scientific, and vaccine hesitancy has emerged as a leading barrier to administering vaccines to protect against COVID-19.
While substantial resources are expended on making biomedical advances, these advances are of little value if people resist or refuse them. The public therefore has a collective interest in sharing the message that vaccines are safe, beneficial, cost-effective, and necessary. More attention must be placed at the intersection of public health, marketing, and education to identify more effective strategies for engaging the general populace in public health efforts, particularly when it comes to preventative measures and/or health-enhancing behavioral changes.
If facts and truth hold less persuasive power than beliefs and values, policy efforts must necessarily concentrate on the latter. Addressing individual and community anti-vaccine attitudes holds the greatest potential to increase the state’s vaccination rate, but, given the prevalence of anti-vaccine sentiment, this will not be easy. As we’ve written previously, the diffusion of vaccine hesitancy is a major threat to public health. Vaccine hesitancy has long affected childhood immunization rates in Michigan, and has left the state below average with regard to the annual flu shot. It is therefore not surprising to see widespread hesitance toward the new coronavirus vaccines.
Vaccine hesitancy is best understood as a wide spectrum of apprehensions and/or beliefs. The source(s) of hesitance in Escanaba, Alpena, or Clare is likely to be quite different from the source(s) of hesitance in Detroit; likewise, neighbors in any of those cities may have different fears about the vaccine and reasons for not yet getting it.
Michigan’s urban/rural (and suburban) divide creates unique challenges to immunization efforts, meaning there’s no one-size-fits all solution. Multifaceted efforts are needed to counter misinformation and ease vaccine concerns or doubts. Ultimately, this means moving away from mass-vaccination sites and shifting to a community-based approach in partnership with local businesses, churches, schools, and social groups. Incentives and mandates offer potential pathways to increase vaccine uptake, but can backfire if people start questioning why, if the vaccine is so good, do we need to bribe and/or force people to get it; policymakers must therefore be careful to ensure the carrot and stick do not transform into a double-edged sword.
Let’s Talk Immunity
Early in the coronavirus pandemic, 70 percent was an estimated threshold for herd immunity to stop the spread of COVID-19. In reality, it’s impossible to predict exactly what the magic number might be that would halt transmission. With virus variants circulating in Michigan and around the globe that are more contagious, a revised threshold of at least 80 percent vaccinated for herd immunity has emerged, though more and more experts assert that herd immunity may no longer be possible.
Some have suggested looking at individuals who have survived COVID-19 together with vaccinated individuals to calculate immunity thresholds, but there are problems with relying on estimates of community infection to create herd immunity to the SARS-CoV-2 virus. Some lasting immunity is conferred after infection, but many questions and uncertainties remain regarding durability of immunity and susceptibility to viral variants. We also don’t know the exact number of community infections, nor precisely how this population overlaps with the number of vaccinated individuals.
Even so, some policymakers have claimed Michigan is already on the verge of achieving herd immunity for COVID-19 based on a wide array of assumptions. Expert analysis does not appear to support this assertion. Moreover, this kind of back-of-the-envelope epidemiology is no way to develop or direct public policy.
Whether or not herd immunity can be achieved, there are limitations to attaching pandemic policy to statewide estimates of herd immunity. Even if 70 percent vaccination turns out to be an adequate target for functional herd immunity, use of a statewide metric belies dramatic differences throughout communities within the state.
High rates of immunization in populous counties like Oakland, Kent, Kalamazoo, and Washtenaw do not ultimately protect rural areas of the state (like Hillsdale, Cass, or Osceola counties) or Detroit where immunizations remain low. While conceptually and theoretically valuable, herd immunity in one community is ostensibly meaningless if transmission and outbreaks are occurring in adjacent communities; this situation will still lead to spillover, resulting in breakthrough infections, reinfections, infection of the vulnerable/immunocompromised, and the continuing possibility for emergent virus mutations that could evade any existing immunity.
The Michigan Department of Health and Human Services has characterized the 70 percent figure as an operational goal, rather than a measure of immunity. It is not clear, however, whether this is because using normal as an incentive to increase vaccine uptake is politically expedient, or because of recognition that, due to ongoing global transmission, the emergence of variants, and the lack of an approved vaccine for children, we may have missed the boat on the possibility of herd immunity.
Still, even absent herd immunity, the virus can be more easily and safely managed with a greater proportion of the population vaccinated, and increasing vaccine uptake is a very worthy policy goal. It remains to be seen if the “Vacc to Normal” challenge will be enough to move the fence-sitters from their perch. When combined with targeted messaging and outreach, as well as efforts to make vaccines more convenient in areas with low uptake, it will have a much better chance at meeting its mark.
Learning from the Pandemic
The Research Council has continually highlighted Michigan’s disinvestment in public health funding; the pernicious politicization of public health issues in recent years gives little hope that this trend will change in any meaningful way. It should be no surprise, therefore, that many of the Greatest Public Health Achievements of the 20th Century—control of infectious diseases (including immunizations), workplace safety, safer and healthier foods, reduction of tobacco use, and healthier mothers and babies—are no longer a given in Michigan.
Public health professionals make decisions, recommendations, and, indeed, issue mandates, based on science, evidence, and historical best-practices. We would all do well to heed this expertise, rather than dismiss, undermine, or attack it. People may argue ad nauseam over the idea that one person’s social contract is another’s tyranny, but they should do so while following scientific guidance to keep themselves and others safe and healthy, including one of the safe and efficacious vaccines for the SARS-CoV-2 virus.
As we move forward, we must learn from our state’s pandemic response (and the strategies of other states and nations) to prepare for the future. We have some successes we can hopefully recreate amid future outbreaks, as well as many failures to analyze and avoid in subsequent epidemic responses. Using this past year of humbling lessons to make systemic policy changes will help us do better than “Vacc to Normal” and refocus public policies to take us “Vacc to the Future.”
